When COVID 19 arrived in Canada I was not surprised to learn that health care workers were getting sick. Even though they were being exposed to a high “viral load,” the reality is that they themselves were in a high risk category because of the health vulnerabilities caused by their work.
For workers who care for the bodies of others, one of the costs of this work is on their own bodies. In the year 2000 I was hired by the Hospital Employees Union, an affiliate of CUPE in B.C., to develop a manual and education program on workplace stress and its impact on the body. HEU’s members include care aides, orderlies, cleaners, food service workers and medical records personnel, both in hospitals and in long term care homes and assisted living facilities. The Workplace Anti-Stress Guide was based on two classic studies of unhealthy work, the Framingham Study on heart disease and the Whitehall Study which linked social hierarchy, stress and health in the workplace. The purpose of our program was to show how the deregulation and privatization of health care had resulted in a level of toxic workplace stress that had significant health impacts on the workers, including musculoskeletal injuries, high blood pressure, diabetes, chronic pain, ulcers, risk of heart disease and a weakened immune system.
Since 2000 working conditions for health care workers have continued to deteriorate as many for – profit companies have moved into and taken over senior care. I write this to hold up care aides, also known as personal support workers or PSW’s, a group whose work has been devalued, underfunded and understaffed. I share the story of the care aides who looked after my mother. She lived in a for -profit facility in Toronto for 9 years, and died there.
Hospitality not Health
In 2004 my brother and I finally moved my 86 year old mother into an assisted-living retirement home. We settled her into her more-than-adequate apartment in the Claremont, an upscale seniors home owned by Revera in “the distinguished Leaside neighbourhood.” On my way out the door I paused to thank the manager in her office. A well dressed blond in her mid fifties, she was very gracious and welcoming to my mother. I was curious about her training, so asked her innocently enough, “ What is your background for this job? Gerontology?” She replied , “No, I have a degree in marketing.” I was shocked but tried to hide it. My heart sank. This was not a good sign that my mother’s health would be a priority in this assisted living facility.
Revera is but one of several for-profit corporations (Sienna, Amica, Chartwell, and Retirement Concepts are some others) operating in Canada, many with shares traded on the stock exchange, who make a profit from the elderly with money. This is pure capitalism with profits coming through the real estate value of their properties and on the backs of workers. My Mom’s facility consisted of “private pay units.” She had inherited money and so she could afford a pricey place like this. Her rented apartment was $7500 a month and included 3 meals a day. There was one day nurse for the entire building of 78 residents , and 24-hour care. This meant care aides/ PSW’s would help residents get to meals, take them to appointments outside the building, and as they became more frail, help them to dress and toilet, as well check in on them in the evening and during the night. The nurse’s job seemed to be mostly about delivering and monitoring each resident’s medications. As the PSW’s had many residents to see on a floor, their time with each resident was limited to a few minutes for the specific task at hand. If a worker phoned in sick they were not replaced. If a resident needed more consistent care it had to be paid for by the resident or their family.
In the ensuing years it became apparent my mother had Alzheimer’s and possibly Parkinson’s disease. The question of diagnosis was problematic as my mother’s doctor had retired, and she was soon terrified to go outside the building, and there was no doctor who served the Claremont. Luckily in 2010, a well–known surgeon and his wife became residents and their son, who was a doctor, offered his services one afternoon a week. He was able to treat my Mom and many others in what was basically a storage room.
Even though this was a retirement residence, where you would suspect , the more frail elderly would move on to long term care, there were many there, like my Mom, who stayed there and were quite ill. The 2008 financial crisis had occurred and it was in Revera’s interest to keep these clients/residents because of the revenue they generated, rather than have empty suites. In order to market the place management kept those who were more ill isolated in their rooms where they had their meals. This made it easier for prospective new residents to experience what was presented more as a country club atmosphere on the main dining floor and the “Happy Hour” patio on the roof. Yet behind the scenes was a situation where many residents needed both the human and physical resources , such as power lifts which move a person from a bed to a wheel chair, of a long term care facility. These residents were encouraged to stay there and hire private care. Not surprisingly, Revera had its own agency – Revera Health Services.
Much of the private care came from the same workers who were already working there on part-time or full time day, evening and night shifts. As well, the agency hired many casual workers who worked short 2-3–hour shifts. The agency took one third of the differing hourly rates we paid for the workers. With real wages tiered, from $13 to $17 an hour, Revera could make more money for profits, which in turn attracted investment. The monthly cost of my mother’s private care, from 7 in the morning to 7 :30 at night, was $7520 plus tax.
RELATIONAL CARE UNDER DIFFICULT CONDITIONS
In the last few years of my mother’s life I would fly in from Montreal or Vancouver every second month and sit in her apartment from morning to evening for four days. There I met and got to know the different care aids who worked with my very Anglo-Irish and very white Mom. There were from many ethnicities – Jamaican, Trinidadian, Eastern European , Latina and Filipino – all women. I found the different people showing up every few hours hard enough for me, never mind my mother, not to mention for the workers, having to learn her routine and complex needs. As my mother’s condition worsened, my brother and I pushed the management so that my Mom would have at least one consistent person to be with her for 5 hours each day. It still meant in a given week there were at least ten other workers who were slotted to be with her, some for 30 minutes, others for two hours.
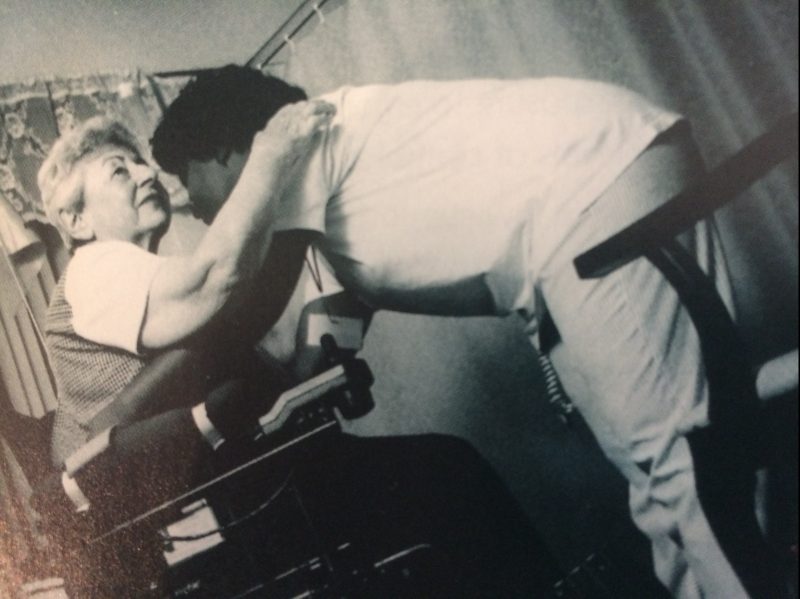
As my mother moved into the later stages of Alzheimer’s the physical work involved in her care increased. A worker had to turn her regularly at night so she wouldn’t get bedsores and in the morning get her out of bed. This involved lifting her, basically a dead weight, into her wheel chair . Only two of the workers could do it on their own; usually a second worker had to be called to help. Eliza was often called because she was strong but she told me she had developed serious back problems over the years and so it was not easy for her. Another physical job was to move my Mom into the seat in the shower and , before she wore diapers, help her onto the toilet. Even to change her diapers, required strength and agility. When my mother was unable to swallow regular food, the worker first had to use a blender to mash her food , and then feed her slowly, three times a day. There were also personal touches. Lila would dress my Mom each morning in bright clothes and brush her hair. Three workers in particular, all Filipina, talked to my Mom a lot, even as she babbled and made no sense. Two called her Moma when they chatted to her, often getting her to smile. As my mother’s body became more rigid as the disease progressed, they would gently hold her hand or stroke her leg. There would always touch, her hair, her hands, her back. They washed her clothes and kept the place clean. When I would arrive I would say “ Hi Mom, it’s your daughter Denise”, and she would look vaguely at me and smile, but I could see that eventually she was regarding Lila, who was with her more, as her daughter.
My Mom’s room became a sort of drop-in for some of the workers. I remember once Mary visited, practically in tears. The woman across the hall, who had Alzheimer’s, had been screaming at her, and this time had started throwing things. The risk of violence is constant for care aides. There was the guy down the hall, younger, in his fifties, who had early onset dementia. They had to keep his door locked as he became prone to fits of violence as he walked in the hall. On another day, Mary came in to report that she had been shifted to kitchen duty for breakfast and lunch, which meant she had to leave home in the suburbs an hour earlier each morning and she had way less time with the residents. As I talked to more of the workers I soon caught a general feeling of malaise as schedules were being constantly shifted and rotation into kitchen and laundry became more frequent. Rather than hire more staff when a worker left, Revera chose to increase the work load of the existing staff.
Besides the workplace stresses of understaffing and low wages, care aides lives outside the job were not easy. Lila had two children and worked during the day; her husband was an orderly and worked at night at a hospital. She had been a nurse in the Philippines. Like most Filipinas she sent money back regularly to her family there. She did not have the time or the money for the two year upgrading course required for foreign nurses to get accredited in Ontario. Mary had been a teacher in the Philippines; she also had young children and a working husband and had to live in the suburbs because rent was too expensive in downtown Toronto. Eliza had been in the military in the Philippines; her children were older, her husband retired, and she needed to work until retirement age in order it support her family here and back home.
On a Sunday night in May, 2013, when I was in Courtenay, B.C., I got a call from the nurse at the Claremont informing me that my mother had pneumonia and she asked me if we wanted her sent to the hospital. I quickly phoned my brother in Nashville and we decided no, that she stay where she was. While she could not communicate how much pain she was in, we had no doubt that the impact of Alzheimer’s on her body was now unbearable and we would let the pneumonia take its natural course. I booked a flight out for the next afternoon. Just before my plane took off, the nurse phoned again to tell me my Mom had died. Lila and Eliza had been with her when she died. Distraught I phoned the apartment and asked Eliza to stay with the body till I arrived at midnight. While I was in shock, the fact that those two women had been with her was somewhat consoling. To my Mom I had been a curious interloper who showed up every few months. They were her regular family. They had provided the emotional care that my brother and I only offered occasionally or on the phone. Many of them came from cultures where elders were valued and who lived their last days with their children. They saw this as work of value and they offered relational care.
Care Workers’ Health First
Julie Rees, Director of Education and Human Rights at HEU, recently said that one of the most stressful jobs in Canada is that of the care aide. In B.C. a care aide job is rated as the most dangerous and high stress, followed by that of police and firefighters. The care aide rates of injury and of PTSD are higher than most occupations, not only because of violence from residents but because of the numbers of deaths they see, especially deaths of people they have become attached to. Care aides’ work is a job that is tasking both physically, emotionally and mentally. Physically it involves lifting, shifting, moving and bathing dead – weight bodies, all within a limited time frame. Mentally they have to be aware of each patient’s needs , their history and behavioural patterns in order to avoid violence. They have to stay alert to notice any change in a resident’s condition and are often the main go-between between the family, food services and nurses. Emotionally, they become attached to patients while having to deal with families and all their emotional needs. Because of privatization, contracting out and deregulation, all for the sake of profit, their work load is unsustainable. The strategy of making many care aides casuals, with less hours of work with no benefits , meant many have had to work two or three jobs. In many privately run homes there are no benefits and sick leave. Underlying all this is systemic racism and sexism, the exploitation of racialized women for the profit of companies mostly run by white people.
COVID 19 has exposed these injustices. There is an opportunity now for justice by restructuring care for seniors. Organizations like CUPE are asking for the elimination of for -profit care and to move seniors care into the public sector, and that this be covered under the Canada Health Act with guaranteed care standards. It is important to include conditions that support the health and safety of care aides. Care aides require not only a just salary with benefits, including paid sick leave and adequate holidays. They need conditions of work that allow them to be healthy. This means having a say in the decisions about what jobs they do and in the care of patients. It means a reasonable workload which can only be met by adequate staffing. And it means ergonomically designed areas of work. It means having enough time for caring contact with patients and support from supervisors and co-workers in all areas of their work. The famous slogan of the Industrial Workers of the World – “an injury to one is an injury to all” has been proven by the pandemic. Now is the time to for all of us to remedy that.

